
Dental Fluorosis and Dental Caries Prevalence among 12 and 15вҖ‘YearвҖ‘Old School Children in Nalgonda District, Andhra Pradesh, India
- *Corresponding Author:
- Dr. Jagadeeswara Rao Sukhabogi
Department of Public Health Dentistry, Government Dental College and Hospital, Hyderabad, Andhra Pradesh, India.
E-mail: jrsukhabogi@yahoo.com
Abstract
Background: Fluoride is a double edged sword. The assessment of dental caries and fluorosis in endemic fluoride areas will facilitate in assessing the relation between fluoride concentrations in water with dental caries, dental fluorosis simultaneously. Aim: The objective of the following study is to assess the dental caries and dental fluorosis prevalence among 12 and 15ГғВўГӮвӮ¬ГӮвҖҳyearГғВўГӮвӮ¬ГӮвҖҳold school children in Nalgonda district, Andhra Pradesh, India. Subjects and Methods: This was a crossГғВўГӮвӮ¬ГӮвҖҳsectional study. Two stage cluster sampling technique was employed to select 20 schools from Nalgonda district. The oral examination of available 12 and 15ГғВўГӮвӮ¬ГӮвҖҳyearГғВўГӮвӮ¬ГӮвҖҳold children fulfilling the inclusion and exclusion criteria was carried out to assess dental caries and fluorosis. The examination was conducted by a single trained and calibrated examiner using the mouth mirror and community periodontal index probe under natural daylight. These areas were divided into four categories, low, medium, high and very high fluoride areas based on the fluoride concentration at the time of statistical analysis. The data was analyzed using Statistical Package for the Social Sciences version 16 (IBM, Chicago, USA). Results: The caries prevalence was less among 12ГғВўГӮвӮ¬ГӮвҖҳyearГғВўГӮвӮ¬ГӮвҖҳold children (39.9% [369/924]) compared with 15ГғВўГӮвӮ¬ГӮвҖҳyearsГғВўГӮвӮ¬ГӮвҖҳold children (46.7% [444/951]). The prevalence was more among females (50.4% [492/977]) than males (35.8% [321/898]). The prevalence was more in low fluoride area (60.5% [300/496]) followed by very high fluoride area (54.8% [201/367]), high fluoride area (32.4% [293/904]) and medium fluoride area (17.6% [19/108]) in the descending order. The fluorosis prevalence increased with increasing fluoride concentration with no difference in gender and age distribution. Conclusion: Low fluoride areas require fluoridation or alternate sources of fluoride, whereas high fluoride areas require defluoridation. Defluoridation of water is an immediate requirement in areas with fluoride concentration of 4 parts per million and above as dental fluorosis is a public health problem in these areas with 100% prevalence.
Keywords
Defluoridation, Dental caries, Dental fluorosis, Endemic fluoride area, Prevalence
Introduction
The recent World Health Organization (WHO) report and other studies suggest dental caries to be a major public health problem in most of the developing countries, affecting 60-90% of the school children in spite of the declining trends in the most developed countries.[1,2] The decline in dental caries among children in highly developed countries started to emerge around 1970 and the percentages of caries free children in different age categories have increased since then. This was mainly attributed to the increased use of fluorides from all sources, especially toothpastes.[3,4] On the other hand, certain developing countries, have reported an increase in dental caries[1,4] The economic, social and political changes in the developing world have had a significant impact on diet and nutrition, with a shift from traditional to a more westernized life-style. This is attributed to increased availability and consumption of refined sugars. There are few resources for curative/restorative intervention and no infrastructure upon which to base large-scale prevention measures. Dental caries is, therefore potentially of major public health significance in developing countries, and the need to focus on its prevention is a matter of urgency.[4,5] India is one among the 25 nations around the globe, showing increasing trends in dental caries and it exists as a smoldering disease that has ingressed its tentacles deep into those regions where there are inadequate resources of dental treatment, lack of public health awareness and motivation and increase in the utilization of refined carbohydrates.[6] National oral health survey and fluoride mapping in India,[7] found the prevalence of dental caries among 12 and 15-year-old children to be 53.8% and 63.1% respectively. A recent study among school going children in an endemic fluoride area in Andhra Pradesh found the prevalence of dental caries among 12 and 15-year-old children to be 55.3% and 57.3%. Prevalence of dental fluorosis was 73% among 12 years and 70.1% among 15 years children.[8] Dental caries and dental fluorosis are two dental diseases among the school children in endemic fluoride areas. Around 17 states in India are endemic to dental fluorosis.[9] Many laboratory, clinical and dental public health researchers after more than 70 years of research have concluded that, fluoride is a double–edged weapon, where its deficiency increases the risk for dental caries and excess consumption in the first 5-10 years of life increases the risk for dental fluorosis.[10]
The fluoride produces a dose-dependent effect on the dentition. However, this is not confined to increased caries resistance. Fluoride causes various disorders, together called as fluorosis, if accumulated above certain levels in the body. According to a WHO report “It may not be possible to achieve effective fluoride based caries prevention without some degree of dental fluorosis.” Public health administrators must seek to maximize caries reduction, whereas minimizing dental fluorosis.[11]
The literature on the relation between fluoride concentration in drinking water with dental caries is conflicting. Some studies reveal an inverse relation[12,13] while others found no relation[14] or a positive association.[15,16]
Nalgonda District in Andhra Pradesh is an endemic fluoride area with fluoride concentration in drinking water ranging from below optimum to optimum and above optimum levels. The district has 1155 revenue villages with 3,359 habitations out of which, 1,122 habitations were identified as fluoride affected.[17] The sparse literature on the relation between dental caries, dental fluorosis with fluoride concentration in drinking water among the school going children in Nalgonda district prompted us for the present study to assess dental caries and dental fluorosis prevalence among 12 and 15-years-old school children in Nalgonda district, Andhra Pradesh, India.
Subjects and Methods
This cross-sectional study was conducted among 12 and 15-year-old school children in Nalgonda district, Andhra Pradesh, India. The study was conducted over a period of 8 months from July 2009 to February 2010. Before the start of the main study, a pilot study was conducted on a convenient sample (n = 100) of school children. The pilot study found the prevalence of dental caries to be 30%. Based on this, the desired sample size was estimated to be 1613 with 95% confidence level and a design effect of five using Master software (Biostatistics Resource and Training Center, Christian Medical College, Vellore).
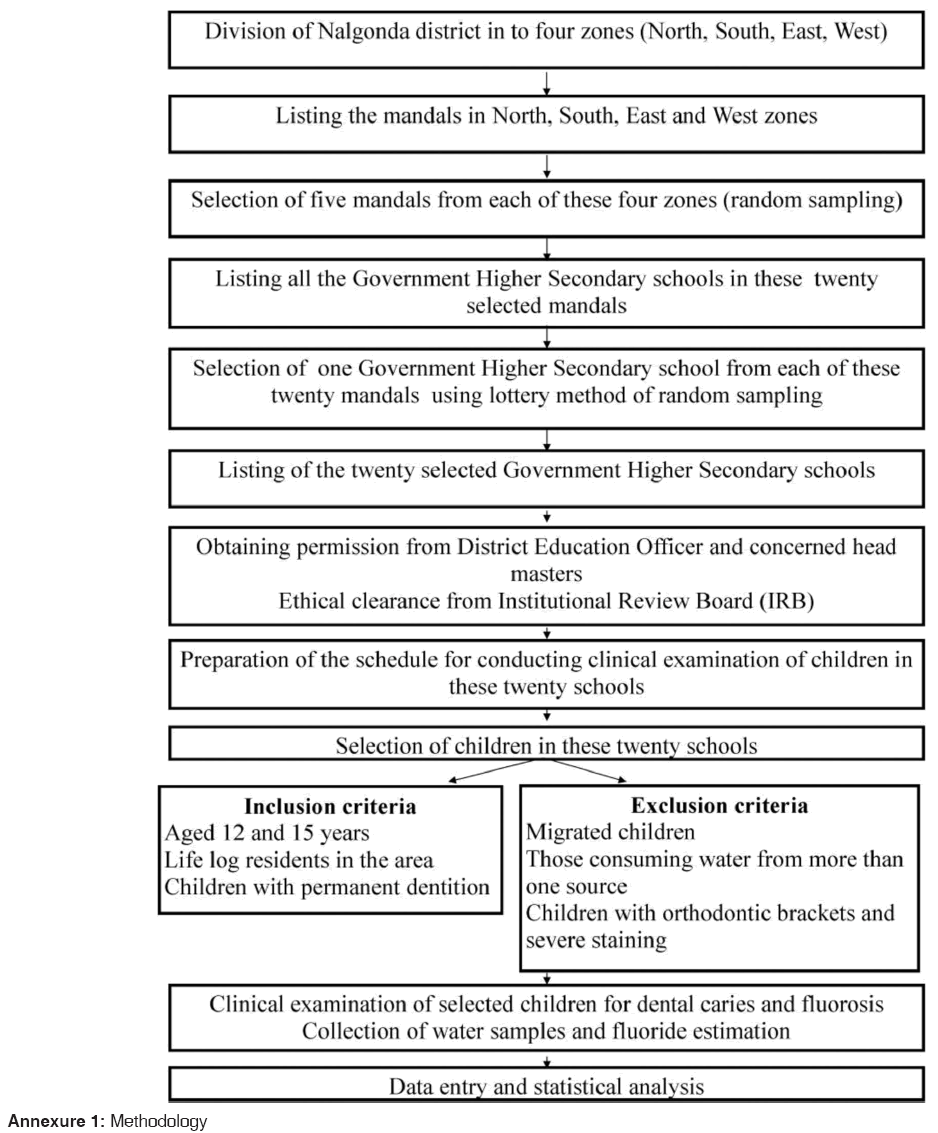
Two stage cluster sampling was used for selection of study participants to the study. Nalgonda district has 59 mandals (administrative divisions) and the district was divided into four zones (North, South, East and West). All the mandals in these zones were listed and five mandals from each of these zones were selected in the first stage. All the government higher secondary schools in these selected mandals were listed. Using this as the sampling frame, one school from each of these 20 mandals was selected using lottery method of simple random sampling. The selected schools were listed and permission to conduct the study in these schools was obtained from the District Education Officer, Nalgonda and concerned head masters. The schedule for conducting the study among these children was prepared and sent to the concerned head masters well in advance. On the day of clinical examination, the list of all grade VI and IX children was procured and the details related to their date of birth were checked. All children from grade VI and IX fulfilling the following inclusion and exclusion criteria were examined in the study.
Inclusion criteria
I. Children aged 12 years and 15 years (those who completed 12 years and 15 years on the day of examination)
II. School children who were lifelong residents in that region and who were using one source of drinking water from birth to at least 10 years of their life
III. Children with all permanent teeth, except third molars, with at least more than 50% of the crown erupted.
Exclusion criteria
I. Children aged less or more than 12 years as well as those aged more or less than 15 years
II. Migrated children from some other place or who were not the permanent residents of the area concerned.
III. Children with a history of drinking water from more than one source in the initial 10 years of their life
IV. Children with orthodontic brackets were excluded as this hindered diagnosis of enamel defects
V. Children with severe extrinsic stains on their teeth in whom assessing fluorosis was not possible.
Ethical clearance for the study was obtained from the Institutional ethics committee, Sri Sai College of Dental Surgery, Vikarabad. A pre-designed structured questionnaire was used to collect the desired information such as oral hygiene practices, diet, sugar exposure, source of drinking water etc., The questionnaire had 15 close ended questions with multiple options to collect information on these aspects. Questionnaire was filled by the investigator by means of face to face interview to avoid misinterpretation of questions and to ensure uniformity in data collection. One trained and calibrated examiner conducted the clinical examination of the selected children using a mouth mirror and community periodontal index probe. The Kappa co-efficient value for intra-examiner reliability was found to be 0.88 for decayed missing filled teeth (DMFT) and 0.81 for dental fluorosis. The agreement was substantial to almost perfect, according to the scale of Landis and Koch.[18] The clinical examination was carried in the school premises under natural day light on the plastic chair after obtaining informed consent from the children and their parents. Participants were made to sit on a chair in an upright position using wall as the head rest, whenever necessary. Dental caries was assessed using Dentition status and treatment needs and dental fluorosis using Dental fluorosis index (WHO oral health surveys).[19]
The first child in the school was requested to obtain 500 ml of water from the source from which children consumed water. The investigator/assistant accompanied the child at the time of collection of water sample. The other samples in the school were collected only when the source of drinking water differed among the children. All the water bottles collected from each school were coded and sent to laboratory for estimation of fluoride concentration. The code written on the water bottle was entered on all the data collection sheets of the children who consumed water from the respective source. This ensured the collection of water samples from all the sources from where the eligible children consumed water during their childhood. The estimation of fluoride concentration in the drinking water was done at “National Institute of Nutrition (Indian Council of Medical Research) Hyderabad using Orion 720 A fluoride meter, coupled with ion specific electrode.
The data was entered onto a personal computer and statistical analysis was done using the statistical package for the social sciences. Inc. version 16, (Chicago, USA). The children were classified into four categories based on the fluoride concentration in the drinking water. This was done at the time of statistical analysis. This ensured that the investigator was not aware about the fluoride concentration in the area at the time when the clinical examination of the children was performed. The four categories were low fluoride area (fluoride concentration <0.7 ppm), medium (0.7-1.2 ppm), high (1.2-4 ppm) and very high fluoride area (4-6.28 ppm). Mean and standard deviation were used to express the quantitative data, while the qualitative data was presented in frequencies and percentages. Kruskal walley’s test was used to compare the difference in the mean DMFT between different categories. The prevalence of dental caries and dental fluorosis was compared using Pearson’s Chi-square test. Spearman’s rho was used to correlate fluoride concentration with dental caries and dental fluorosis. The statistical significance was fixed at 0.05. The autoclaved set of instruments was used for oral examination of the children. The methodology employed in the study is diagrammatically depicted in Annexure 1.
Results
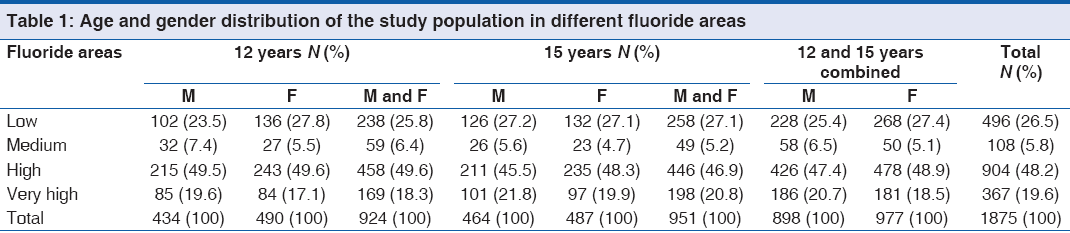
A total of 1875 school children were examined in the present study. The gender distribution of the study population in different fluoride areas is denoted in Table 1.
Dental caries prevalence
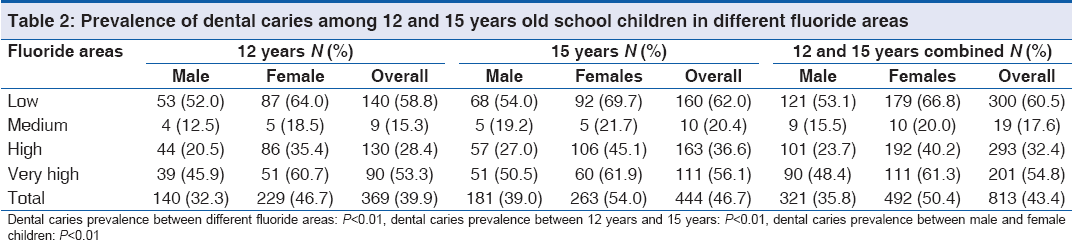
The overall prevalence of dental caries among the school children was 43.4% (813/1875). The prevalence of dental caries was significantly higher among females (50.4% [492/977] compared with males (35.8% [321/898]). The prevalence was more among 15-years-old children (46.7% [444/951] compared with 12 years children (39.9% [369/924]). The prevalence of dental caries among children in low fluoride areas was 60.5% [300/496] followed by very high fluoride area (54.8% [201/367]), high fluoride area (32.4% [293/904]) and medium fluoride area (17.6% [19/108]). The difference in the prevalence of dental caries between different fluoride areas was statistically significant. These results were true even when the comparison was made separately among 12 and 15 years old children [Table 2].
Dental fluorosis prevalence
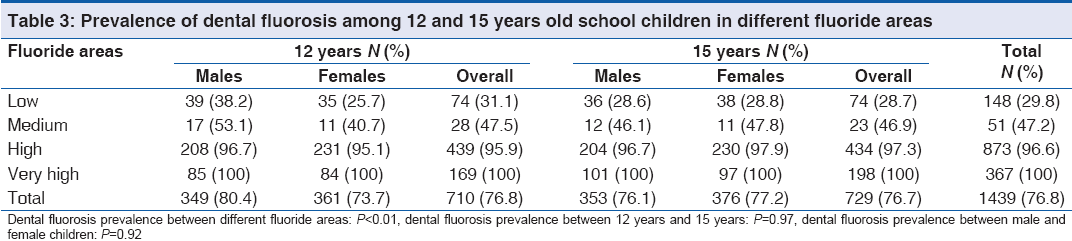
The prevalence of dental fluorosis was 76.8%. There was no statistically significant difference in the prevalence of dental fluorosis between 12 and 15-years-old children. There were no gender differences in the prevalence of dental fluorosis. The prevalence of dental fluorosis significantly increased with increasing fluoride concentration. The prevalence of dental fluorosis in very high, high, medium and low fluoride areas was 100% (367/367), 96.6% (873/904), 47.2% (51/108) and 29.8% (148/496) respectively. These results were true even when a separate comparison was made between different fluoride areas among 12 and 15-year-old children [Table 3].
Correlation between fluoride concentrations in water and dental caries, dental fluorosis
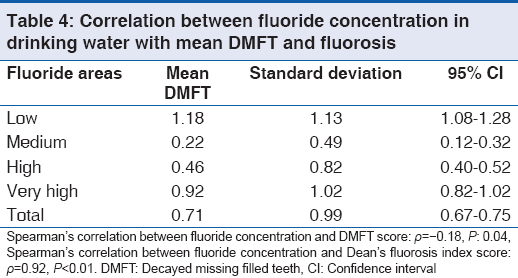
The mean DMFT score was lowest in the medium fluoride area (0.22 [0.49]). The mean DMFT score in high fluoride area, very high fluoride area and low fluoride area was 0.46 (0.82), 0.92 (1.02) and 1.18 (1.13) respectively. The difference in the mean DMFT score between different fluoride areas was statistically significant [P < 0.01, Table 4]. A negative correlation (Spearman’s P = −0.18) was noted between fluoride concentration in drinking water and mean DMFT score. A positive correlation (Spearman’s P = 0.92) was observed between dental fluorosis index score and fluoride concentration. There was no statistically significant difference in relation to dietary habits, oral hygiene aids used, frequency of brushing and frequency of sugar consumption among the school children in different fluoride areas.
Discussion
The scanty published literature on the prevalence of dental caries and fluorosis among school children in endemic fluoride areas, which provide the best opportunity in assessing the relation between increasing fluoride concentration on both these diseases prompted us to undertake the present study. The study was conducted among 12 and 15-year-old school children in Nalgonda district, Andhra Pradesh, India. The WHO in its manual on basic oral surveys (1994)[19] has specified 5, 12, 15, 35-44 and 65-74 years as index age groups for assessing the oral health status. Among these, 12 years is considered the global monitoring age for international comparison of dental caries and 15 years represent the other adolescent age group. Moreover, these are the two age groups for obtaining a reliable sample from the school system. This prompted us in the selection of 12 and 15-years-old school children as the study participants in the present study.
The prevalence of dental caries was least in medium fluoride area followed by high fluoride area. The prevalence was highest in low fluoride area followed by very high fluoride areas. The mean DMFT value was also least in medium fluoride area. The highest mean DMFT was noted among children in low fluoride area followed by very high fluoride area and high fluoride area in the descending order. This clearly suggests that fluoride in drinking water offer maximum protection against dental caries at optimal concentration which ranges from 0.7 to 1.2 parts per million (ppm) according to previously published literature.[8] The fluoride concentration below optimal as well as above optimal was found to be harmful. A study by Shekar et al.[8] among 12 and 15-years-old children in Nalgonda district, Andhra Pradesh found the prevalence of dental caries to be highest in areas where the concentration of fluoride in drinking water was less than 0.7 ppm followed by areas with fluoride concentration of 4.1 ppm and above. The results of the present study were consistent with the findings of this study. Murray JJ (2003)[20] quoted a study by Torell and Ericsson assessing the use of fluorides in different forms for caries prevention. The study found the frequent exposure to low concentration fluoride solution to be more protective than infrequent exposure to high concentration fluorides. The continuous exposure of the teeth to water containing optimum and slightly above optimum levels of fluoride may facilitate remineralization of incipient carious lesions through topical effect. The optimum fluoride concentration though may result in milder forms of dental fluorosis will not alter the surface texture of the teeth at these concentrations. The fluoride concentrations above 4 ppm may result in severe dental fluorosis which manifest as confluent pitting.[20] The alteration in the surface texture favors food retention and plaque accumulation, which in turn may increase the risk for dental caries in areas where the concentration of fluoride is above 4 ppm. The lack of protective benefit and pitting caused by severe dental fluorosis explain the high caries prevalence in low and very high fluoride areas respectively. Reddy and Tewari.[21] conducted a study among 1750 school children in the age group 12-17 years in Bhatinda district of Punjab, India. The prevalence of dental caries in areas with the fluoride concentrations of 0.3, 1.1, 2, 3.4, 5.4 and 10.4 ppm was 89.0, 61.2, 54.7, 72.8 73.6 and 85.5% respectively. The study found highest caries prevalence in low fluoride areas (0.3 ppm) and very high fluoride areas (10.4 ppm). The results of our study were consistent with the findings of this study and others.[15,22-28]
We found a higher prevalence of dental caries among females compared with males. In the absence of dietary differences, the higher caries prevalence among females is attributed to early eruption of teeth among females and thereby longer exposure to deleterious oral environment.[29] The body surface area among males is more than that for females. Due to greater physical activity, boys consume more water than compared to girls. The frequent water consumption results in frequent exposure of teeth to fluoridated water and higher level of protection among boys compared to girls. A study by Singh and Singh[30] among school going children in Patna found the prevalence to be high in female children (52.6%) than males (50.2%). The results of our study were in agreement with this study and others.[31]
The irreversible nature of the disease and longer exposure of teeth to deleterious oral environment may explain the higher caries prevalence of caries among 15 years group compared to 12 years group. National oral health survey and fluoride mapping in India[7] found the overall prevalence of dental caries to be increasing with increasing age. Our results were consistent with the results of national oral health survey in India.
The overall prevalence of dental caries among 12 and 15-year-old children in the present study was significantly less compared to prevalence noted in National oral health survey in India for these age groups. Our study was conducted in an endemic fluoride belt and hence, the less caries experience among children in our study compared to data at national level may be attributed to protective action of fluoride in drinking water.
The increasing prevalence and severity of dental fluorosis with increasing fluoride concentration may be explained by the fact that dental fluorosis is a developmental defect which occur because of exposure to water containing high fluoride concentrations. This relation between water fluoride concentration and severity of dental fluorosis is dose dependent with increasing concentration leading to higher risk.[32] A positive correlation between fluoride concentration and dental fluorosis indexscore was found in many epidemiological studies in the past.[25,33,34] our results were consistent with all these studies.
Dental fluorosis is a developmental defect affecting the teeth before calcification (before 10 years of age). The exposure to higher fluoride concentrations after the calcification (which is complete by 10 years of age for all permanent teeth except third molars) might not increase the severity of dental fluorosis. This explains the lack of age and gender predilection for dental fluorosis in the present study. Chandrashekar and Anuradha[35] in their study on the prevalence of dental fluorosis in rural areas of Davangere, India found no age predilection for dental fluorosis. Our results were in agreement with this study and others.[36]
The number of children in medium fluoride areas in the present study was significantly less compared to other categories. The fluoride categories were made at the time of statistical analysis based on fluoride concentration in drinking water and not at the time of selection of study participants. This clearly suggests that the optimal fluoride areas are less in number even in an endemic fluoride belt. Many areas were having either below optimal fluoride concentration or above optimal levels. This might have resulted in less number of children in medium fluoride areas. The finding highlights the need for a comprehensive fluoride mapping in endemic fluoride belts and remedial actions based on fluoride concentrations in water. The less number of children in medium fluoride area compared to others might have influenced the difference between different fluoride areas to some extent, which needs to be further evaluated in future studies.
Summary and Conclusion
The present study found high caries prevalence in low and high fluoride areas with fluoride concentrations lesser than 0.7 ppm and higher than 4 ppm. The medium fluoride area with optimum fluoride concentration (0.7-1.2 ppm) had the lowest caries prevalence. The prevalence of caries was more among females compared to males. 15-years-old children had more caries prevalence than 12 years. There was a positive correlation between fluoride concentration and prevalence of dental fluorosis with no age and gender predilection. The results strongly support the findings of previous studies conducted in endemic fluoride areas that increase in the fluoride concentration above optimal levels does not offer additional benefits in caries prevention. But, instead, increase the risk for dental fluorosis. A defluoridation plant was installed in Nalgonda by National Environmental Engineering and Research Institute, Nagpur. This community defluoridation technique is popularly known among dental fraternity in India as Nalgonda technique of defluoridation. The defluoridation plant is presently abandoned due to lack of maintenance. This reflects the negligent attitude among the policy makers towards dental diseases. The results of this study and previously conducted studies highlight the immediate need for defluoridation at least in areas with fluoride concentration above 2 ppm. Here, dental fluorosis is a major public health problem than dental caries as the prevalence is almost 100%. The high caries prevalence in low fluoride areas call for water fluoridation and or other alternate strategies for caries prevention. The running and maintenance of defluoridation plants is more expensive than the fluoridation plants. Determined efforts with public private partnership can translate these idealistic goals into realistic ones. The professional organizations such as Dental Council of India and Indian Dental Association should strongly support water fluoridation in low fluoride areas and defluoridation in high fluoride areas to combat two dental diseases related to fluoride concentrations in drinking water.
Acknowledgments
I would like to thank the Principal and management of Sri Sai College of Dental Surgery for their continuous support and encouragement for undertaking this project. We thank the District Education Officer, Nalgonda, The Head masters of the schools concerned and the participants for their kind co-operation.
References
- Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ 2005;83:661-9.
- Petersen PE, Lennon MA. Effective use of fluorides for the prevention of dental caries in the 21st century: The WHO approach. Community Dent Oral Epidemiol 2004;32:319-21.
- Marthaler TM. Changes in dental caries 1953-2003. Caries Res 2004;38:173-81.
- World Health Organization. Educational Imperatives for Oral Health Personnel: Change or Decay? Geneva: WHO; 1990.
- Bagramian RA, Garcia-Godoy F, Volpe AR. The global increase in dental caries. A pending public health crisis. Am J Dent 2009;22:3-8.
- Kulkami SS, Deshpande SD. Caries prevalence and treatment needs in 11-15 year old children of Belgaum city. J Indian Soc Pedod Prev Dent 2002;20:12-5.
- National Oral Health Survey and Fluoride Mapping. An epidemiological study of oral health problems and estimation of fluoride levels in drinking water. New Delhi: Dental Council of India; 2004.
- Shekar C, Cheluvaiah MB, Namile D. Prevalence of dental caries and dental fluorosis among 12 and 15 years old school children in relation to fluoride concentration in drinking water in an endemic fluoride belt of Andhra Pradesh. Indian J Public Health 2012;56:122-8.
- Suthar S, Garg VK, Jangir S, Kaur S, Goswami N, Singh S. Fluoride contamination in drinking water in rural habitations of northern Rajasthan, India. Environ Monit Assess 2008;145:1-6.
- Hiremath SS. Fluorides. Text Book of Preventive and Community Dentistry. 2nd ed. New Delhi: Reed Elsevier India Private Ltd.; 2011. p. 370-402.
- Ruan JP, Yang ZQ, Wang ZL, Astrøm AN, Bårdsen A, Bjorvatn K. Dental fluorosis and dental caries in permanent teeth: Rural schoolchildren in high-fluoride areas in the Shaanxi province, China. Acta Odontol Scand 2005;63:258-65.
- Fejerskov O, Larsen MJ, Richards A, Baelum V. Dental tissue effects of fluoride. Adv Dent Res 1994;8:15-31.
- Horowitz HS, Heifetz SB, Meyers RJ, Driscoll WS, Korts DC. Evaluation of a combination of self-administered fluoride procedures for control of dental caries in a non-fluoride area: Findings after 2 years. Caries Res 1977;11:178-85.
- Grobler SR, van Wyk CW, Kotze D. Relationship between enamel fluoride levels, degree of fluorosis and caries experience in communities with a nearly optimal and a high fluoride level in the drinking water. Caries Res 1986;20:284-8.
- Grobleri SR, Louw AJ, van Kotze TJ. Dental fluorosis and caries experience in relation to three different drinking water fluoride levels in South Africa. Int J Paediatr Dent 2001;11:372-9.
- Olsson B. Dental findings in high-fluoride areas in Ethiopia. Community Dent Oral Epidemiol 1979;7:51-6.
- Serving the people of Nalgonda. Nalgonda.org. Available from: http://www.nalgonda.org/fluorosis/fluoridelevels.htm. [Last cited on 2013 Aug 24].
- Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977;33:159-74.
- World Health Organization. Assessment form. Oral Health Surveys, Basic Methods. 4th ed. Geneva: WHO; 1997. p. 21-51.
- Murray JJ, Nunn JH, Steele JG. Fluorides and dental caries. The Prevention of Oral Diseases. 4th ed. New York: Oxford University Press; 2003. p. 35-60.
- Subba Reddy VV, Tewari A. Prevalence of dental caries to different levels of fluoride in drinking water. J Indian Dent Assoc 1992;63:455-9.
- El-Nadeef MA, Honkala E. Fluorosis in relation to fluoride levels in water in central Nigeria. Community Dent Oral Epidemiol 1998;26:26-30.
- Driscoll WS, Horowitz HS, Meyers RJ, Heifetz SB, Kingman A, Zimmerman ER. Prevalence of dental caries and dental fluorosis in areas with negligible, optimal, and above-optimal fluoride concentrations in drinking water. J Am Dent Assoc 1986;113:29-33.
- Ekanayake L, van der Hoek W. Dental caries and developmental defects of enamel in relation to fluoride levels in drinking water in an arid area of Sri Lanka. Caries Res 2002;36:398-404.
- Mann J, Tibi M, Sgan-Cohen HD. Fluorosis and caries prevalence in a community drinking above-optimal fluoridated water. Community Dent Oral Epidemiol 1987;15:293-5.
- Elías-Boneta AR, Psoter W, Elías-Viera AE, Jiménez P, Toro C. Relationship between dental caries experience (DMFS) and dental fluorosis in 12-year-old Puerto Ricans. Community Dent Health 2006;23:244-50.
- Pontigo-Loyola AP, Medina-Solis CE, Borges-Yañez SA, Patiño-Marín N, Islas-Márquez A, Maupome G. Prevalence and severity of dental caries in adolescents aged 12 and 15 living in communities with various fluoride concentrations. J Public Health Dent 2007;67:8-13.
- Ibrahim YE, Affan AA, Bjorvatn K. Prevalence of dental fluorosis in Sudanese children from two villages with 0.25 and 2.56 ppm fluoride in the drinking water. Int J Paediatr Dent 1995;5:223-9.
- Khan AA, Jain SK, Shrivastav A. Prevalence of dental caries among the population of Gwalior (India) in relation of different associated factors. Eur J Dent 2008;2:81-5.
- Singh DK, Singh RP. Prevalence of dental caries in school going children of Patna. J Indian Dent Assoc 1981;53:267.
- Demirci M, Tuncer S, Yuceokur AA. Prevalence of caries on individual tooth surfaces and its distribution by age and gender in university clinic patients. Eur J Dent 2010;4:270-9.
- Srivastava AK, Singh A, Yadav S, Mathur A. Endemic dental and skeletal fluorosis: Effects of high ground water fluoride in some North Indian Villages. Int J Oral Maxillofac Pathol 2011;2:7-12.
- Sampaio FC, Hossain AN, von der Fehr FR, Arneberg P. Dental caries and sugar intake of children from rural areas with different water fluoride levels in Paraíba, Brazil. Community Dent Oral Epidemiol 2000;28:307-13.
- Kumar J, Swango P, Haley V, Green E. Intra-oral distribution of dental fluorosis in Newburgh and Kingston, New York. J Dent Res 2000;79:1508-13.
- Chandrashekar J, Anuradha KP. Prevalence of dental fluorosis in rural areas of Davangere, India. Int Dent J 2004;54:235-9.
- GopalakrishnanP, VasanRS, SarmaPS, NairKS, ThankappanKR. Prevalence of dental fluorosis and associated risk factors in Alappuzha district, Kerala. Natl Med J India 1999;12:99-103.



 The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.
The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.