
Knowledge, Attitude and Practices of Women Towards Breast Cancer in Benin City, Nigeria
- *Corresponding Author:
- Mr. Samuel O. Azubuike
Department of Public/Community Health, Novena University, Ogume, Delta State, Nigeria
E-mail: samonaz2000@yahoo.com
Abstract
Background: Breast cancer is the principal cause of cancer deaths among women worldwide. African women in comparison with their low incidence of cancer, disproportionately bear a high cancer mortality rate. Aim: The study was aimed at investigating level of breast cancer awareness, attitudes and practices towards early detection strategies. Subjects and Methods: The study was conducted in Oredo municipal council of Benin city and adopted a descriptive cross sectional design. Purposive, stratified and simple random sampling were used to select 365 women from 9 health facilities in 6 wards of the municipality. Self‑administered questionnaires were used. Analysis was done using Social Science Statistical Package, version 16 (United States, 2007) (country of make and if). Test of associations employed chi square statistical tool with level of significance generally taken at 0.05. Results: About 90.5% (314/347) knew about breast cancer, but only about 49.71% (172/347) knew up to 3 breast cancer risk factors. A total of 65.2% (226/347) could identify up to two breast cancer signs and symptoms. While about 56.5% (195/347) knew at least one early detection strategy, it was however only about 17.73% (61/347) that practiced regularly at least one of the early detective procedures. Practice of early detection strategies was significantly associated with knowledge (P = 0.01 respectively). Conclusion: The result shows that while substantial number still remains ignorant of breast cancer issues, a good number of those who have knowledge were yet to translate knowledge and attitudes into practice.
Keywords
Attitude, Awareness, Breast cancer, Knowledge, Nigeria, Practice
Introduction
African women; in comparison with their low incidence of cancer disproportionately bears a high cancer mortality rates.[1] It has been estimated that by the year 2020, approximately 70% of new cancer cases will occur among individuals in developing countries and population groups that have previously enjoyed low incidence, with a substantial fraction likely to be breast malignancies.[2-4] This is complicated by late presentation that generally characterise cancer diagnosis among Nigerian and other African women, with about 70-90% presenting late, hence diminishing survival probabilities compounded by exorbitant cost.[1,5-8] The peak age of breast cancer in Nigeria is about ten years earlier than the experience of many western women.[5,9,10] This could be attributed to increasing adoption of western life style and diet [1] compounded by poor knowledge and attitude related to cancer issues. Breast Cancer awareness and attitude has been described as a common denominator to Several factors determining the stage at which patients with breast cancer present to the hospital.[8] There are reports suggesting that factors related to women’s knowledge and beliefs about breast cancer and its management may contribute significantly to medical help-seeking behaviours.[4,11,12] One potentially important strategy in reducing breast cancer mortality is the use of screening to achieve earlier detection of cancer.[13] Early diagnosis usually results in treatment before metastasis and signifies a better outcome of management.[14]
A few studies on Knowledge, attitude and practices towards breast cancer has been conducted in Benin City Nigeria.[4,10] Each of these studies have recorded low knowledge and attitude among the participants. The need for new studies especially in the core urban part of the city has become necessary to ascertain levels of improvement. This would be necessary in designing appropriate awareness creation intervention strategies. Knowledge of the level of awareness and attitude among urban population would also give an indication of what may be expected in the rural areas, since urban people are expected to have more access to information. It is against this backdrop that this study has undertaken to study Breast Cancer knowledge, Attitudes, Practices and its hindrances among women in Benin City.
Subjects and Methods
The study was a cross-sectional design carried out for a period of 3 months. It involved women of reproductive age (19-49 years) attending Immunization Clinic in Oredo local, Government, Benin City, Nigeria. The specified age group is at risk since reports had it that breast cancer tends to occur among African patients at a younger age with peak incidence between 35-45 years of age within the west African region.[1] The sample size of 365 was calculated based on result of previous similar study.[4]A confidence interval of 95%, absolute precision of 0.05 were used.
Purposive, stratified and simple random Sampling techniques were used. Seven wards out of 12 wards were purposively selected based on strategic locations and population sizes. The sample was stratified based on population strength or proportion of each ward. In each ward, specific health centres were purposefully selected based on their catchment population which was also used as a basis for determining the sample to be studied in each ward. At each health facility simple random sampling was used in selecting individual subjects included in the study starting from the first eligible person met at the health facility. It was only women of reproductive age met at the immunisation clinics during the period of the study that were chosen.
The study was approved by the Department of Public and Community Health, Novena University. Written permissions were obtained from health facilities selected, while the informed consents of respondents were obtained orally.
A semi-structured questionnaire comprising of 23 questions covering socio-demographic information, knowledge, attitude and practice of the respondent. It was developed based on questions used in previous peer reviewed published studies and those selected based on discretion.
The questionnaires were self-administered to the women at the clinic, however special assistance were given to women were not sufficiently literate. The completed questionnaires were collected on the spot by the researcher. The questionnaire was seen by senior researchers in the department of public and Community health, Novena University. The data was analyzed using Statistical Package for Social Sciences (SPSS), version 16 (United States, 2007). Test of associations employed chi square statistical tool with level of significance generally taken at 0.05. Knowledge of breast cancer risk factors was further analyzed by assigning 1 to each positive answer (Yes) to knowledge of each of the 11 breast cancer risk factors tested, and ‘0’ to each negative answer (No). The sum obtained by each respondent ranging from 0 to 11 was used in assessing level of knowledge. This also was applied to knowledge of breast cancer signs and symptom where expected sum ranged from 0 to 7. For the ‘Levels of practice of early detection preventive strategies’ (breast self-examination, clinical breast examination, and Mammography), three options were given, ‘Yes’, ‘No’ and ‘Irregular practice’. Each ‘yes’ answer was assigned a score of 2, each ‘Irregular’ answer was assigned a score of 1 while each ‘No’ answer was given a score of 0. Practice was graded from 0-poor (‘No’ answer for the three) to 6-very good (‘Yes’ answer for the three).
Results
About 347 questionnaires were retrieved out of 365 distributed given a response rate of 95.1% which was considered good for the study. According to Table 1, more than half of the respondents, 56.5% (196/347) was aged below 30 years; Dominant occupations were Business and civil service. About 75.8% (263/347) have either secondary or tertiary education; while about 12.7% (44/347) have previous history of breast cancer. Moreover result on general knowledge of breast cancer shows that about 90.5% (314/347) have heard or read about bread cancer, while about 76.3% (267/347) knew that breast cancer is the commonest cancer among women compared to 21.3% (74/347) who did not know.
| Variable | Frequency (%) |
|---|---|
| Age | |
| 15-19 | 25(7.2) |
| 20-24 | 67(19.3) |
| 25-29 | 104 (30) |
| 30-34 | 91(26.2) |
| 35-40 | 38 (11) |
| >40 | 22(6.3) |
| Total | 347 (100) |
| Marital status | |
| Single | 63(18.2) |
| Married | 280(80.7) |
| Divorced | 3(0.9) |
| Widow | 1(0.3) |
| Religion | |
| Christianity | 319(91.9) |
| Muslim | 20(5.8) |
| Traditional | 8(2.3) |
| Total | 347 |
| Occupation | |
| Civil servant | 84(24.2) |
| Business | 112(32.3) |
| Farming | 8(2.3) |
| Artisan | 27(7.8) |
| Student | 54(15.6) |
| Professional | 22(6.3) |
| Fulltime housewife | 37(10.7) |
| Others | 3(0.9) |
| Total | 347 (100) |
| Level of education | |
| <primary | 8(2.3) |
| Secondary | 143(41.2) |
| Tertiary | 120(34.6) |
| Others | 14(4.0) |
| Total | 347 (100) |
Table 1: Socio demographic data
Figure 1 shows that greater number 39.8% (138/347) whose scores ranged 3-5 (knowledge of 3-5 risk factors) had fair knowledge. While 26.0% (90/347) who scored 0 (no knowledge of any of the risk factors) had very poor knowledge compared to 0.8% (3/347) that had a very good knowledge. Generally it was only about 49.7% (172/347) that knew up to 3 breast cancer risk factors.

Figure 1: Figure
Table 2 shows 25.1% (87/347) with scores, 2-3 and 4-5 respectively have fair and good knowledge respectively, of breast cancer signs/symptoms. A significant number 22.5% (78/347) with score῾0’ have very poor knowledge compared to 15% (52/347) with 6-7 scores that have a very good knowledge. A total of 50.2% (174/347) have fairly good knowledge (ie knowledge of at least two breast cancer signs and symptoms). According to the same table, Many, about 91.6% (319/347) were of the opinion that breast cancer could be cured if detected early, However it was only about 28.8% (101/347) that strongly agreed with the opinion. Similarly while about 89.6% (311/347) favoured the opinion that early detection strategies are effective in detecting breast cancer, it was only about 3.4% (120/347) that strongly agreed with it. The greatest reason given for non practice were ‘the feeling that they cannot have cancer’, 22.5% (78/347), followed by lack of awareness and forgetfulness (19.3% respectively, (67/347), Unwillingness to be examined by a male doctor was the least reason (2.6%).
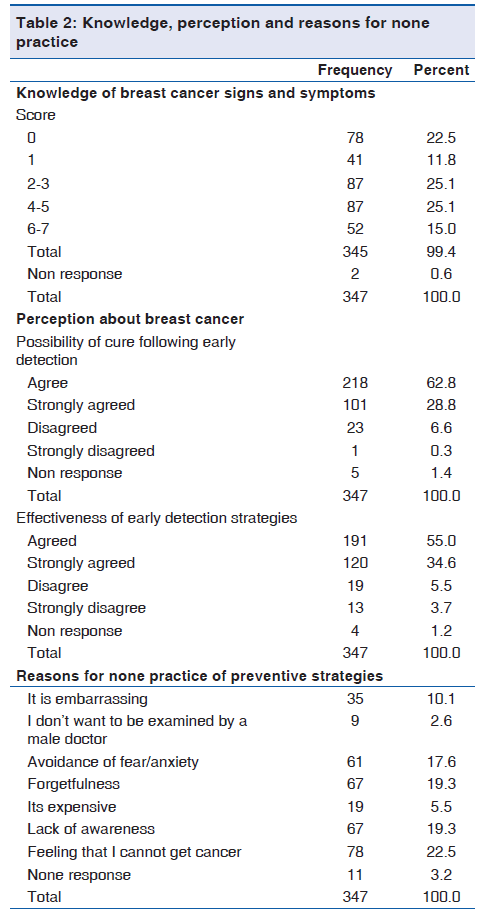
Figure 2 shows that majority, 43.4% (150/347) have poor knowledge compared to only 16.5% (57/347) that had very good knowledge. However a total of 56.5% (195/347) could identify at least one of the secondary preventive procedures.

Figure 2: Knowledge of breast cancer early detection strategies
The figure shows that 53.4% (184/347) have poor level of practice, 17.7% (61/347) has fairly good practice (Practiced one regularly or at least two irregularly) and 7.2% (25/347) has very good practice (Practiced at least two regularly).
The Relationship between knowledge and practice
There was a very strong association between knowledge and practice of preventive strategies (P < 0.01). Similarly also It seems that the higher the knowledge level, the higher the tendency to practice any of the early preventive procedures (P < 0.01).
Discussion
The result suggests that a good number may be enlightened t since reasonable percentage possessed tertiary education. Studies suggest that people with higher education tend to have better knowledge and practices towards breast cancer prevention.[15] More so the result shows that only 12.7% (44/347) had previous history of breast cancer. Positive personal history about breast problem has been associated with willingness to practice precautionary measures.[16]
According to the result, most of the respondents knew about breast cancer with less number however correctly stating that it is the commonest cancer among women. These were high compared to only 78% that knew about breast cancer in previous study [17] and 61-63.6% that stated that it was commonest among women in other studies.[4,16] This may be due to increasing effort on awareness campaign in Nigeria in the past few years especially in the urban areas, or possibly due to the fact that a fair number had tertiary education which has been reported to be positively associated with better knowledge and attitude.[15]
Figure 1 indicates that only 49.7% (172/347) has fairly good knowledge of breast cancer risk factors, being able to identify up to 3 breast cancer risk factors. This findings was higher compared to finding of Okobia, et al., 2006 and Saludeen and friends in 2009 (21.4% and 36.7% respectively).[4,18] Gakwaya, et al. (2008) reported that more than 50% of female subjects did not know about risk factors of breast cancer.[19] However, good and fair knowledge (35% and 40% respectively) were reported in Pakistan,[20] but the respondents were nurses. Despite the fairly good report of this study, it is still worrisome that about 26% had no knowledge of any Breast cancer risk factor. Knowledge of breast cancer signs and symptoms according to Table 2 could be said to be fairly good. Previous studies in Nigeria have indicated lower knowledge with only 21.4% and 1.9% respectively being able to identify painless lump as a sign.[4,21] While this may suggest increased awareness over time, it is disturbing that about 22.5% (78/347) were still in the dark about all the seven signs and symptoms of breast cancer. Timely presentation has been linked to ability to recognize breast cancer signs/symptoms.[22,23]
In relation to knowledge of the preventive strategies-BSE, CBE and mammography, Figure 3 shows that majority could not identify any of them. The number affected was high compared to the number that could not identify any breast cancer risk factor, as well as the specified signs/symptoms. However, with 56.5% (196/347) who knew at least one method of early detection preventive practice, this knowledge could be said to be fairly good. A study among non-professionals and undergraduate students reported 61.4% for BSE.[24] Gakwaya, 2008 reported low knowledge of Mammography (71%).[19] The need for awareness program in relation to early preventive strategies is obvious.[25]

Figure 3: Level of practice of early detection strategies
Most of the respondents were of the opinion that breast cancer could be cured if detected early. This is in consistent with related studies among nurses in general hospital Lagos, Nigeria where about 78.4% of the respondents agreed that breast cancer is curable if diagnosed and treated early.[11] This study further revealed that a relatively good number saw early screening procedures as effective in detecting breast cancer. Similar perception was also reported in Ibadan Nigeria.[21] While this may suggest a good attitude towards early detection procedures, the low percentage of those whose opinion were strong deserves attention.
In relation to level of practice, Figure 3 showed that more than half had poor practice, having not been practicing any of the three preventive measures. About 17.7% (61/347) who had fairly good practice, practiced at least one regularly, while only about 7.2% (25/347) practiced at least two regularly. Generally, this indicates that practice is low compared to the total number who knew at least one method of preventive practice. Previous studies have reported low practice levels, for BSE (34.9%) and CBE (9.1%), and no history of practice for Mammography.[4]
Where Practice of mammography has been reported, it has been very low.[19,26,27] Generally this finding indicates that presence of knowledge and positive opinions towards preventive strategies should not be interpreted as readiness to practice secondary preventive strategies.
The commonest reason reported for not practicing any of the preventive procedures was the ‘feeling that one cannot get breast cancer’, followed by ‘lack of awareness and forgetfulness’ then ‘avoidance of fear and anxiety’. Similar reasons were also given in a previous studies study.[28,29] Specifically ‘the feeling that one cannot get breast cancer’ indicates disbelief and superstition. Disbelief and misconception about breast cancer has been reported as contributory factor to late reporting.[30]
A very strong association seems to exist between knowledge and practice of early detection strategies. Even though not all who knew about the preventive strategies practiced it, there is a very strong indication that practice increases as level of knowledge increases Another very strong association between the knowledge of breast cancer risk factors and practice of preventive strategies was observed. Knowledge of the risk factors seems to be motivational to practice, probably because it helps people to estimate to what extent they are vulnerable. Previous studies have also identified relationship between knowledge and practice of preventive procedures.[16]
Conclusively, the study shows that there is good level of awareness of breast cancer among the respondents. However this level of awareness was not consistent in all issues related to breast cancer. Moreover a comparatively small but substantial number remain ignorant of breast cancer issues. While tendency for positive attitude toward preventive practice could be said to be high, there still exist some superstitious beliefs and ignorance that could hinder good practice among some.
While there is a strong relationship between knowledge and practice, it seems that Knowledge would not always translate to practice in all cases. The need for a more focused cancer education is obvious.
Study limitation
One limitation of this study was that the women of reproductive age included were only those attending immunisation clinics within the period of the study; hence their experience may not fully reflect what may be obtainable in the general population.
Relationship between knowledge and practice
General knowledge and practice of early detection strategies was extremely significant (χ2 = 1.556, df = 9, P = 0.001)
Knowledge of risk factors and practice of early detection strategies was also extremely significant (χ2 = 63.3, df = 6, P = 0.001)
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Fregene A, Newman LA. Breast cancer in sub-Saharan Africa: How does it relate to breast cancer in African-American women. Cancer 2005;103:1540-50.
- Jones SB. Cancer in developing world: A call to action. BMJ 1999;319:505-8.
- World Health Organization. Mortality by sex, cause, and WHO Region, estimate for 1998. In: The World Health Organization Report 1999. Geneva: WHO; 1999.
- Okobia MN, Bunker CH, Okonofua FE, Osime U. Knowledge, attitude and practice of Nigerian women towards breast cancer: A cross-sectional study. World J Surg Oncol 2006;4:11.
- Anyanwu SN. Breast cancer in eastern Nigeria: A ten year review. West Afr J Med 2000;19:120-5.
- Amir H, Azizi MR, Makwaya CK, Jessan S. TNM classification and breast cancer in an African population: A descriptive study. Cent Afr J Med 1997;43:357-9.
- Okobia MN, Osime U. Clinicopathological study of carcinoma of the breast in Benin City. Afr J Reprod Health 2000;5:56-62.
- Muguti GI. Experience with breast cancer in Zimbabwe. J R Coll Surg Edinb 1999;38:75-8.
- Ihekwaba FN. Breast cancer in Nigerian women. Br J Surg 1992;79:771-5.
- Osime OC, Okojie O, Aigbekaen ET, Aigbekaen IJ. Knowledge attitude and practice about breast cancer among civil servants in Benin City, Nigeria. Ann Afr Med 2008;7:192-7. Available from: http://www.annalsafrmed. org/text.asp?2008/7/4/192/55654. [Last accessed on 2011 Apr 19].
- Odusanya OO, Tayo OO. Breast cancer knowledge, attitude and practice among nurses in Lagos Nigeria. Acta Oncol 2001;40:844-8.
- Hadi MA, Hassali MA, Shafie AA, Awaisu A. Evaluation of breast cancer awareness among female University students in Malaysia. Pharm Pract (Internet) 2010;8:29-34.
- Parkin DM, Whelan SL, Ferlay J, Raymond L, Young J. Cancer incidence in five continents. Vill Lyon L: ARC Press; 1997.
- American Cancer society. Breast cancer, facts and Figures 2008;9. Available from: http://www.cancer. org/. [Last accessed on 2011 Apr 19].
- Adebamowo CA, Ajayi OO. Breast cancer in Nigeria. West Afr J Med 2000;19:179-91.
- Haji-Mahmoodi M, Montazeri A, Jarvandi S, Ebrahimi M, Haghighat S, Harirchi I. Breast self-examination: Knowledge, attitudes, and practices among female health care workers in Tehran, Iran. Breast J 2002;8:222-5.
- Montazeri A, Vahdaninia M, Harirchi L, Harirchi AM, Sajadian A, Khaleghi F. Breast cancer in Iran: Need for greater women awareness of warning signs and effective screening methods. Asia Pac Fam Med 2008;7:6. Available from: http://www.apfmj.com/content/7/1/6. [Last accessed on 2011 Apr 19].
- Salaudeen AG, Akande TM, Musa OI. Knowledge and attitude to Breast cancer and breast self examination among female undergraduate. Eur J Soc Sci 2009;7:157-65.
- Gakwaya A, Galukande M, Luwaga A, Jombwe J, Faulal J, Kiguil-Malwadde E, et al. Breast cancer guidelines for Uganda (2nd Edition 2008). Afr Health Sci 2008;8:126-32.
- Ahmed F, Mahmud S, Hatcher J, Khan SM. Breast cancer risk factors knowledge among nurses in a teaching hospital of Karachi, Parkistan: A cross-sectional study. BMC Nurs 2006;5:6.
- Abimbola OO, Oladepo O. Knowledge of breast cancer and its early detection measures among rural women in Akinyele Local Government Area, Ibadan, Nigeria. BMC Cancer 2006;6:271.
- Uche EE. Cancer awareness among a Nigerian population. Trop Doct 1999;29:39-40.
- Odusanya OO. Breast cancer: Knowledge, attitude and practices of female schoolteachers in Lagos, Nigeria. Breast J 2001;7:171-5.
- Augustus M, Adeyinka A, Chenyelu O. Breast Self Examination among non professionals in Nigeria. Niger J Surg Sci 2005;15:74-7.
- Smith RA, Caleffim M, Albert US, Chen TH, Duffy SW, Franceschi D, et al. Global summit early detection and access to care panel. Breast cancer in limited resources countries: Early detection and access to care. Breast J 2006;12:S16-26.
- Alam AA. Knowledge of breast cancer and its risk and protective factors among women in Riyadh. Ann Saudi Med 2006;26:272-7.
- Zincir H. The knowledge and behavior about breast cancer in 40 year old and older women in Malatya province. (Ph.D. Thesis). Malatya: Inonu University, Institute of Health Sciences; 2000.
- Secginli S, Nahcivan N. Breast cancer screening behavior among women. Proceeding of the 2nd International and 9th National Nursing Congress; Antalya/Turkey, 07–11 September 2003.
- Muhammed SM. Knowledge, Attitude and Practice Regarding Breast Cancer among Medical Students. Bangladesh (A master’s thesis protocol studies) University Umea: Department of Public Health and Clinical Studies; 2007. Available from: http://www.cancer.gov/cancertopics/ pdq/treatment/breast/patient/page 2. [Last accessed on 2007].
- Luquis RR, Cruz IJ. Knowledge, attitude and perceptions about breast cancer and breast cancer screening among Hispanic women residing in South Central Pennsylvania. J Community Health 2006;31:25-42.



 The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.
The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.