
Morbidity and Mortality Pattern of Childhood Illnesses Seen at the Children Emergency Unit of Federal Medical Center, Asaba, Nigeria
- *Corresponding Author:
- Dr. Bertilla U Ezeonwu
Department of Pediatrics, Federal Medical Center, Asaba, Delta State, Nigeria.
E-mail: uzovin@yahoo.com
Abstract
Background: Morbidity and mortality from childhood illnesses has remained a major point of interest globally. Malaria, respiratory tract infection and diarrheal diseases are the leading causes of childhood morbidity and mortality. Aim: The aim of the following study is to determine the pattern of morbidity and mortality of children seen at the children emergency room of a tertiary hospital, Federal Medical Center in Asaba, Nigeria. Subjects and Methods: A descriptive study of post‑neonatal childhood admissions over a 5 year period (January 2007‑December 2011) was undertaken. Information obtained included age, gender, diagnosis, month of admission and outcome. Descriptive and inferential statistics were used to analyze the demographic characteristics of the patients and associations with outcome variables. Results: A total of 3,830 children with aged ranges between 1 month and 180 months were admitted within this period of study from January 2007 to December 2011: 2,189 males (57.2%, 2189/3830) and 1,641 (42.8%, 1641/3830) females. More than 70% (2912/3830) were under 5 years of age. The common indications for admission were malaria (30.3%, 1159/3830), diarrheal diseases (20.4%, 780/3830), respiratory tract infections (RTIs) (19.0%, 728/3830) and sepsis (4.4%, 168/3830). There were 221 (5.8%, 221/3830) deaths and more deaths were recorded in children <12 months of age, P < 0.01. Major causes of death were complicated malaria (24.4%, 54/221), sepsis (19.9%, 44/221), diarrheal diseases (18.1%, 40/221) and RTIs (7.7%, 17/221). Conclusion: Preventable infections are the major causes of morbidity and mortality in CHER and children <5 years of age are commonly affected.
Keywords
Asaba, Children, Diarrhea, Malaria, Respiratory infections
Introduction
Preventable diseases such as, pneumonia, diarrheal diseases and malaria are major causes of childhood morbidity and mortality world-wide.[1,2] The State of the World’s Children 2012 report showed that globally, 7.6 million children under 5 years of age die annually and 3.7 million deaths occur in Sub-Saharan Africa.[3] In Nigeria, under five mortality rate as of 2010 was 143.[3] Family poverty and illiteracy are significant underlying risk factors, so also are overcrowding, unsafe drinking water and unsalutary sanitary habits.[1,2] Pneumonia, diarrhea and malaria account for 41% of annual death globally and 49% in Africa.[2] The bulk of childhood morbidity and mortality affect mainly children under 5 years of age.[1,2,4] Several studies in Africa reported infectious diseases as the leading causes of childhood death.[5-11] These diseases can be prevented, and the treatment is accessible and affordable.[1] For children who are 5 years and older, non-communicable[4,12] were the most common causes of death.
The children emergency room (CHER) is the first point of contact for children who need urgent medical care before they are discharged home or sent to the ward for completion of treatment. The knowledge of the pattern of morbidity and mortality in CHER helps in evaluating and improving the existing facilities.[6,7] There has been no such study in this tertiary health facility. Therefore, this index study is timely as it will help to appraise the facilities on the ground and provide data for future re-evaluation. The knowledge will also help in designing protocols for the proper management of the common ailments presenting in CHER of this center, health education and advocacy as it may apply.
Subjects and Methods
The study was carried out at the Federal Medical Center (FMC), located in Asaba, the capital of Delta State of Nigeria. Asaba is in the rain forest region of Nigeria with wet (rainy) and dry seasons. Rainy season includes the months of April through October while the dry season spans from November to March.[13]
The CHER of FMC Asaba is a 7-bed facility and receives patients from Delta State and its neighboring states in Nigeria. It runs on a 24 h basis with consultants, residents, nurses and record staff. Acute illnesses in children 1-180 months (15 years) are managed within the facility before transfer to the appropriate unit.
The current report is a descriptive review of all the admissions from January 2007 to December 2011 (inclusive). Ethical approval was obtained from the Ethics Committee of FMC Asaba. All medical case records of eligible subjects were analyzed. The eligibility criteria were: Presentation at the emergency unit, documentation of the date and month of admission, age, gender, diagnosis and outcome of management (defined as discharged home, transferred to the ward, discharged against medical advice or died).
Diagnosis of the diseases was done by the attending doctors based on the clinical features and available laboratory results. For comorbidities, children with more than one disease were grouped together depending on the doctor’s primary and secondary diagnoses.
Data obtained were analyzed using the statistical package for social science version 20.0 for Windows® (IBM Inc, Chicago Illinois, USA 2011) and Epi Info version 3.4.3 (CDC Atlanta, USA 1997). Continuous variables were analyzed and expressed as means and standard deviations (SDs). Categorical variables were compared using the Chi-square test and significant level was set at P < 0.05.
Results
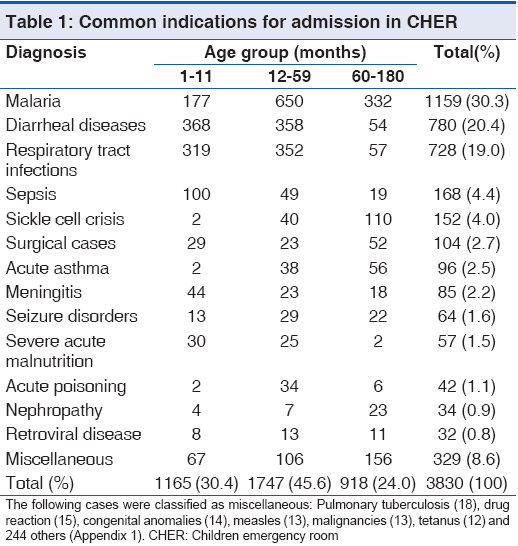
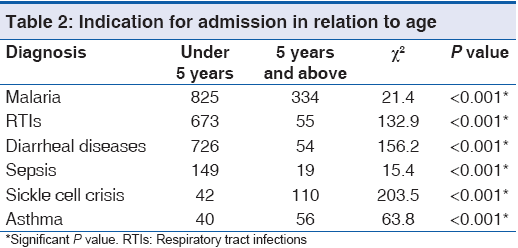
Within the 5 year review period, a total of 3890 children aged between 1 and 180 months (15 years) were admitted in CHER: 3830 (98.5%, 3830/3890) with complete data sets were included in the analysis. There were 2,189 males (57.2%, 2189/3830) giving a male:female ratio of 1.3:1. The mean (SD) age of the subjects was 39.3 (45.0) months (95% confidence interval, 37.9-40.8, P < 0.01). As you can see in Table 1, the subpopulation of children aged below 5 years was 2,912 (76.0%, 2912/3830), whereas children 5 years and above was 918 (24.0%, 918/3830). The common indications for admission were malaria (30.3%, 1159/3830), diarrheal diseases (20.4%, 780/3830) and RTIs (RTIs, 19.0%, 728/3830), making up 69.7% (2667/3850) of the total number of admissions, [Table 1]. For those with RTIs, the proportions of those with the various forms of the disease were: Bronchopneumonia 36.1% (262/728), pharyngotonsillitis 33.1% (241/728), bronchiolitis 18.1% (132/728), rhinitis 8.2% (60/728), lobar pneumonia 2.6% (19/728) and acute otitis media 1.9% (14/728). Malaria, diarrheal diseases, RTIs and sepsis predominated in children <5 years old while sickle cell crisis and acute asthmatic attacks were common among children aged 5 years and above [Table 2].
With regards to seasonal variation, more cases were admitted during the rainy season 2,161 (56.4%, 2161/3850) than the dry season 1,669 (43.6%, 1669/3830): P < 0.01. Admissions due to malaria and RTIs were higher during the rainy season while those due to diarrheal diseases were more during the dry season. About 85% (36/42) of accidental poisoning cases occurred in children <5 years and 57.1% (24/42) were males. Kerosene ingestion was the most common (45.2%, 19/42) followed by alcohol intoxication (19.0%, 8/42). Table 3 shows the distribution of cases with co-morbidities with 141 (3.7%, 141/3830) of the children being affected by more than one disease condition.
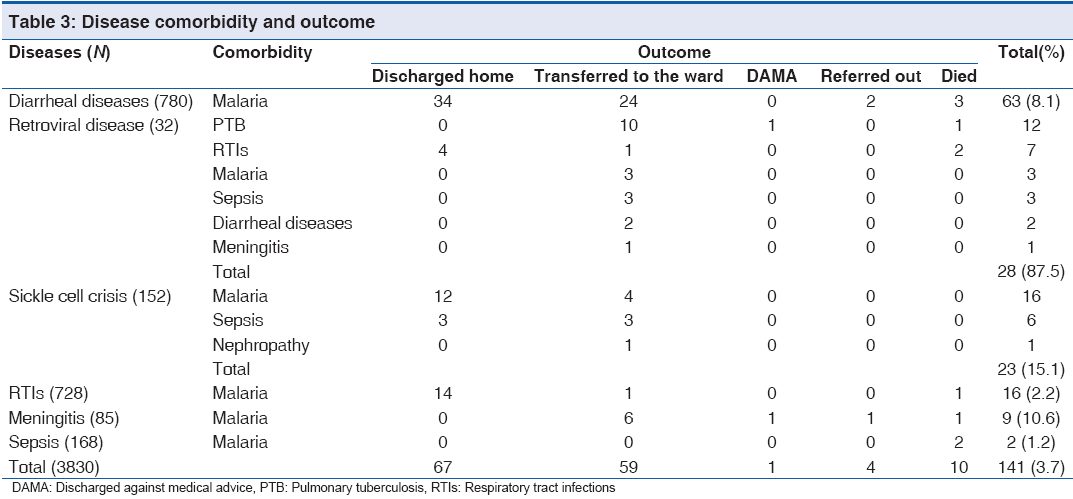
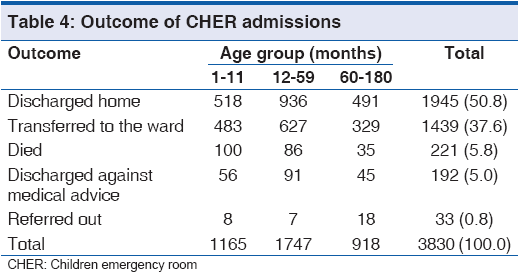
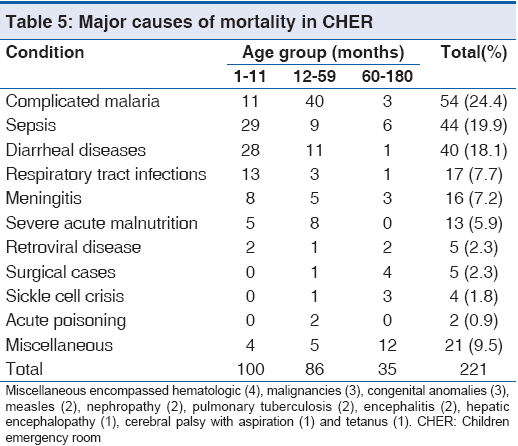
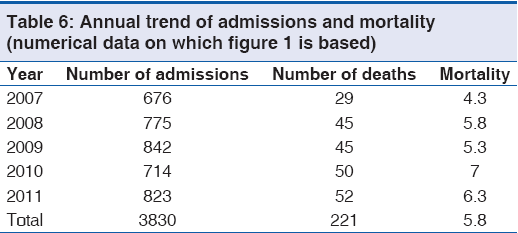
Majority of cases, 50.7% (1,945/3830) were discharged home while 221 deaths were recorded giving overall mortality rate of 5.8%, 221/3830 as shown in Table 4. Totally 100 children died at <1 year of age constituting about 45% (100/221). More than 80% (186/221) of deaths occurred in children <5 years of age P < 0.01. As shown in Table 5, major causes of death were complicated malaria (24.4%, 54/221), sepsis (19.9%, 44/221), diarrheal diseases (18.1%, 40/221) and RTIs (7.7%, 17/221) and severe anemia was found in greater than 50% (35/54) of cases of complicated malaria. While death due to complicated malaria was more prominent in children 12-59 months, death due to sepsis, diarrheal diseases and RTIs occurred more in infants. Only 10 (7.1%. 10/141) of cases with concomitant diseases died and death was more among those with diarrhea, as shown in Table 3. Diarrheal diseases caused more deaths during the dry season P < 0.01. Annual mortality rate in CHER ranged from 4.3% to 7.0%, [Figure 1 and Table 6] whereas overall mortality is 5.8% (221/3830).

Figure 1: Annual trend of admissions and mortality
Discussion
The findings of the review showed that preventable diseases remain the greatest contributors to childhood morbidity and mortality in our facility in consonance with World Health Organization (WHO) report.[1] Our findings share similarity in morbidity and mortality patterns with various studies done in different centers in Nigeria over a period between 2002 and 2011.[6-8] Specifically, malaria, pneumonia and diarrheal diseases continue to dominate as the most common causes of morbidity and mortality among children under 5 years of age. However, non-communicable diseases like sickle cell crisis and acute asthma contribute more to morbidity and mortality in older children. The comorbid conditions observed in the review were associated with infectious diseases malaria and respiratory diseases. These diseases are reportedly the common diseases in children in the developing countries are thus not unexpected to coexist with other diseases. Children with human immunodeficiency virus acquired immune deficiency syndrome had the worst impact with pulmonary infections, notably tuberculosis, contributing more to the morbidity rate in the group. Much morbidity and mortality due to tuberculosis has been shown to occur more in children.[14] These studies[6-8] have illustrated the persistence of infections as the main cause of childhood morbidity and mortality over time in Nigeria.
The persistence of malaria as a prominent childhood problem, despite control strategies give credence to reports of poor uptake of the multiple control measures for malaria has not been appreciable. It is therefore not unexpected that the disease still plays a significant role in childhood morbidity and mortality in the country. Only 42% of Nigerian households have at least one insecticide treated net (ITN) while 29% of children under 5 years are actually sleeping under ITN.[3] These figures are too small to significantly reduce the incidence of malaria. The WHO reported a 27% decline in malaria parasitaemia in Burkina Faso following an increase in ITN coverage from 22% to 73%.[15] The use of ITN should be supported with improvement of the sanitary condition in Nigeria as this review showed that morbidity and mortality due to malaria were more during the wet season, when the mosquito breeding places are rejuvenated. Drainage of stagnant pools of water that serve as a breeding place for the malaria vector and promotion of the use of ITN will act synergistically to reduce the morbidity due to malaria. Contribution of complicated malaria and sepsis to the mortality ratio is appreciable and quite significant. These cases are indicative of poor health sector effectiveness, which if well-structured, would aid early detection and intervention thus stemming the scourge. In Namibia and Botswana where effective health systems are in place, significant reduction in malaria case fatalities have been recorded.[15] Preventive measures and improvement of health delivery have been shown in Tanzania and Uganda to improve outcomes using the basic health tools such as integrated management of childhood illnesses (IMCI).[16] Furthermore in India and Bangladesh the introduction of early detection and treatment of childhood illnesses through the use of IMCI modules have significantly reduced the morbidity and mortality of these childhood illnesses.[16] In contrast, Nigeria started implementation of IMCI in 1997 but still has a high under five mortality rate.[3]
Risk factors for the persistence of the RTIs and diarrhea as causes of mortality in under-5 children, include malnutrition, poor breastfeeding, overcrowded living condition, low immunization coverage and low birth weight, poor personal hygiene, unavailability of portable water and efficient waste disposal systems.[1,5,6] Interestingly, this study showed that the menace of diarrheal diseases is more during the dry season: When the temporary sources of water supply in many communities are exhausted. In Nigeria the health indices still remain abysmal due to the failure of the health system for instance, there is significant numbers of children who are still stunted and wasted, few children are exclusively breastfed[3] further demonstrating the presence of the risk factors to pneumonias and diarrheas. Effective preventive measures such as vaccination against Streptococcus pneumoniae[3] and Rotavirus are yet to be included in the routine Nigerian national immunization programs.[3] The weak health system notably in the absence of well-equipped facilities and also poor patient transfer system are major contributors to the morbidly and mortality rates.
Similar to the findings by Adejuyigbe et al.,[17] children with acute poisoning were majorly those under 5 years of age, mostly of male gender and kerosene ingestion was the most common. Overcrowding with limited space for proper storage of household chemicals like kerosene, storage of such chemicals in attractive containers may have played some roles.
The review noted an appreciable proportion of children dying from the non-communicable diseases, significantly in children 5 years and above. The development of immunity to common childhood diseases such as malaria and rotavirus in the older children as well as an introduction of vaccines against other preventable childhood diseases can explain the trend away from communicable disease as observed from the review.[18] The high morbidity ratios of diseases such as asthma, sickle cell anemia noted in this review has not changed from the observations made in several studies.[19] The implication is that less attention is still paid to these diseases, which will continue to impact of children if not reversed. Asthma is showing increasing incidence in the developing parts of the world and constituting an important factor in daily-adjusted life year’s indices of the populations.[20] This review has shown that such non-communicable diseases, which are often chronic, cause appreciable morbidity and should be controlled to improve the quality of life of the individuals.
The findings of this review although showing similarity to other studies still shares the limitation associated with hospital-based studies which are the restrictions in the extrapolation of the outcome to the general population. Furthermore the lack of pathological confirmation of causes of death may affect some of the probable causes of death.
Conclusion
Preventable diseases still constitute the major cause of morbidly and mortality in our facility and children <5 years of age are commonly affected. Improvement of the social and health system may impact to reduce the incidence of these diseases and their impact on the health of children.
Acknowledgment
We are grateful to the nurses in children emergency room, FMC Asaba who kept the admission registers and the medical records officers who retrieved the case notes.
Source of Support
Nil.
Conflict of Interest
None declared.
References
- World Health Organization. Children: Reducing mortality. Fact sheet number 178. Available online at http://www. who.int/mediacentre/factsheets/fs178/en/index.html. [Last accessed on 2013 Dec 10].
- UNICEF, WHO. Countdown to 2015Decade Report(2000-2010): Taking Stock of Maternal, Newborn and Child Survival. Available online at http://www.countdown2015mnch.org. [Last accessed on 2012 Jul 20].
- UNCEF. The State of the World’s Children 2012. Statistical Tables. 2012. p. 81-138. Available online at http://www. unicef.org/sowc2012/Last accessed on 2012 August 22
- World Health Organization. Six diseases cause 90% of infectious disease deaths. World Health Organ Infectious Disease Report. 1999. Available from: http://www.who. int/infectious-disease-report/ch1.text.html. [Last on 2008 Dec 22].
- Olumide YM, Odubanjo MO. Reducing child mortality in Nigeria (Workshop Report) [Internet]. Lagos The Nigerian Academy of Sciences, West African Book Publishers 2009. [Last accessed on 2012 Dec 4]. Available from http://www. nas.org.org/index.php?option=com.
- Abhulimhen-Iyoha BI, Okolo AA. Morbidity and mortality of childhood illnesses at the emergency paediatric unit of the University of Benin Teaching Hospital, Benin City. Niger J Paediatr 2012;39:71-4.
- Ibeziako SN, Ibekwe RC. Pattern and outcome of admissions in children’s emergency room of the University of Nigerian Teaching Hospital Enugu. Niger J Paediatr 2002;29:103-7.
- Onyiriuka AN. Morbidity and mortality patterns of post neonatal paediatric medical admissions in a large mission hospital in Benin City, Nigeria. J Med Biomed Res 2005;4:49-58.
- Sacarlal J, Nhacolo AQ, Sigaúque B, Nhalungo DA, Abacassamo F, Sacoor CN, et al. A 10 year study of the cause of death in children under 15 years in Manhiça, Mozambique. BMC Public Health 2009;9:67.
- Shamebo D, Muhe L, Sandström A, Wall S. The Butajira rural health project in Ethiopia: Mortality pattern of the under fives. J Trop Pediatr 1991;37:254-61.
- Omokhodion FO, Oyemade A, Sridar MK. Morbidity pattern among under five children of market women in Ibadan. Niger J Med 2003;30:135-9.
- George IO, Alex-Hart BA, Frank-Briggs AI. Mortality pattern in children: A hospital based study in Nigeria. Int J Biomed Sci 2009;5:369-72.
- Bommie O. Lands and climate. Motherland Nigeria geography. Available from: http://www.motherlandnigeria. com. [Last accessed on 2013 Feb 7].
- Cruz AT, Starke JR. Pediatric tuberculosis. Pediatr Rev 2010;31:13-25.
- Elliott EJ. Acute gastroenteritis in children. BMJ 2007;334:35-40.
- Armstrong Schellenberg J, Bryce J, de Savigny D, Lambrechts T, Mbuya C, Mgalula L, et al. The effect of Integrated Management of Childhood Illness on observed quality of care of under-fives in rural Tanzania. Health Policy Plan 2004;19:1-10.
- Adejuyigbe EA, Onayade AA, Senbanjo IO, Oseni SE. Childhood poisoning at the Obafemi Awolowo University Teaching Hospital, Ile-Ife, Nigeria. Niger J Med 2002;11:183-6.
- World Malaria Report 2011. Ch. 7. Geneva: World Health Organization; 2011. p. 51-79. Available from: http://www. who.int/malaria/world malaria report 2011/WMR2011. [Last accessed on 2013 Apr 9].
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2197-223.
- Asher MI, Montefort S, Björkstén B, Lai CK, Strachan DP, Weiland SK, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet 2006;368:733-43.



 The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.
The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.