
The Role of Complications of Community Acquired Pneumonia on the Outcome of the Illness: A Prospective Observational Study in a Tertiary Institution in Eastern Nigeria
- *Corresponding Author:
- Dr. Godwin C Mbata
Department of Medicine, Federal Medical Centre, Owerri, PMB 1010 Owerri, Imo State Nigeria.
E-mail: mbatag@yahoo.com
Abstract
Background: Community acquired pneumonia (CAP) is a major cause of mortality and morbidity in our environment. Recent data on the role of complications on outcome of CAP are not readily available in Nigeria. Aim: This study aims to analyze the influence of complications on the outcome of CAP in a tertiary health center in Eastern Nigeria. Subjects and Methods: A prospective observational study was carried out on 80 patients with CAP, who met the inclusion criteria. Data relating to their age, gender, and clinical details; severity assessment using CURB 65 (C‑ confusion, Serum urea > 7mmol/L, R‑respiratory rate > 30, B‑systolic BP > 90 and diastolic BP ≤ 60, age > 65 years.) scoring system, laboratory results, complications, and outcome (mortality) were collected. The statistical package used for data analysis is SPSS version 17.0 (Chicago IL USA). Data were presented in tables and charts. Sample means, standard deviation, and Chi‑square test were used for statistical significance. Severity was assessed using CURB65 scoring system. Outcome of interest was 30 day mortality. In all P value of 0.05 was regarded as significant. Results: Eighty patients were recruited for the study, 39 males and 41 females; giving male:female ratio of 1:1.05. The mean age range was 56 (18.0) years. A total of 37 patients were managed as out‑patients while 43 were managed as in‑patients. Complications were observed in 25 patients. Severe hemodynamic changes and pleural effusion 8/25 (32%) were the most common complications observed. Total mortality was 12/80 (15%). Mortality was higher in in‑patients than out‑patients however, this was not statistically significant. Mortality in those with complications was 6/25 (24%) compared to 6/55 (11%) in those without complications (P = 0.10). Conclusion: Mortality rate in patients with CAP though higher in patients with complications numerically were not found to be significantly higher than in those without complications. We posit that other factors like presence of higher severity assessment scores (CURB‑65 scores) and co‑morbidities may be more important predictors of mortality in CAP patients and should be further studied.
Keywords
Community acquired pneumonia, Complications, Eastern Nigeria, Mortality, Outcome
Introduction
Community acquired pneumonia (CAP) is an infectious cause of death world-wide, including, Nigeria and other developing nations.[1-3] There is little documentation on CAP in Nigeria however, the work carried out more than three decades ago in Western part of the country showed that about 20% of patients with CAP will die.[4] A more recent work in the Western Nigeria[5] has however revealed a rate of 26% among admitted patients with CAP. A hospital study carried out two decades ago recorded mortality of 21.7%[2] in the South-Eastern Nigeria while a recent study in Eastern Nigeria[6] showed mortality to be 11.9%; which is still unacceptably high in our environment. CAP is the 6th or 7th cause of death in the USA, the number one cause of infection related death and the reason for more than one million hospital admissions.[7]
Complications commonly occur in CAP and they are even more common when diagnosis is delayed due to late presentation, initial incorrect diagnosis or wrong choice of initial antibiotics. Complications are more frequently associated with bacterial than viral pneumonia. Important complications include, massive pleural effusion, serious hypotension that produces severe hemodynamic changes, lung abscess, lung cavitation, sepsis with attendant shock, and acute respiratory failure.[2,4,8] These complications may be severe and life threatening. Other complications include mild confusion, mild jaundice, hemoptysis, mild anemia, and arthritis, which are rarely of any clinical consequences. The role of these complications on outcome of CAP has been studied in different regions of the world giving variable results.[2,4,8,9] The need to document the role of complications on the outcome of our CAP patients has necessitated this study, since early identification of these complications and managing them along with the CAP will improve the outcome of patients with CAP in our environment.
Furthermore, this study aims to compare the mortality outcome of the patients with complications and those without complications.
Subjects and Methods
Study design and patients
Data were collected prospectively from consecutively recruited patients with CAP seen at the Accident and Emergency unit, Medical out-patients unit and medical wards of the University of Nigeria Teaching Hospital (UNTH). All patients with both clinical and radiological diagnosis of CAP seen from December 2008 to June 2009 were enrolled for study, if they met inclusion criteria. Ethical clearance was obtained from ethics Committee of the UNTH Enugu.
Study area
The study area was the UNTH Enugu Nigeria. The institution is a tertiary health institution with 750 bed spaces, which serves Enugu, majority of the South-Eastern towns and some parts of middle belt states of Nigeria. The hospital serves over one million people and sees over 6,000 patients annually. About 2.02% of these patents are treated for CAP annually.[6]
Definitions of terms
CAP was defined as an acute infection of the pulmonary parenchyma that was associated with symptoms and signs of acute infection followed by the presence of an acute infiltrate on chest radiograph in a patient who has not resided in a hospital or health-care facility in the previous 14 days.[3,10] All the patients were assessed by specialist physician before admission and by a specialist respiratory physician before discharge. The final diagnosis was made by a respiratory physician and was based on the clinical, radiological and laboratory results.
Severe hemodynamic change was defined in this context as systolic BP < 90 or diastolic BP ≤ 60 and requiring fluid resuscitation (B of CURB-65 score).
Pleural effusion was defined as mild when it was only detected on chest X-ray and not symptomatic, while massive effusion was symptomatic, detected clinically and seen on chest X-ray.
Sepsis was defined when blood culture yielded organisms and involvement of additional organ other than the lungs and septic shock with clinical features of shock.
Patients with CAP were classified into low, intermediate, and high-risk groups according to british thoracic society (BTS) CURB-65 scoring system.[11,12]
Inclusion and exclusion criteria
All consenting adults ≥ 18 years were included in the study. Exclusion criteria included those admitted to the hospital in the previous 14 days, patients whose symptoms develop greater than 48 h following admission, patients with tuberculosis (TB) or previous chest X-ray, which may conflict with diagnosis of CAP; and patients who were unwilling to participate.
Outcome measure
The primary outcome was the 30 day all-cause mortality.
Data collection
A standard questionnaire designed to cover personal data and review symptoms of CAP were used for the study. Data collected during subject assessment included age, gender, and co morbidities. Documented physical signs included pulse rate, axillary temperature, respiratory rate, and blood pressure. Blood pressure was checked prior to intravenous fluid resuscitation or inotropic support.[3,13] Both systolic and diastolic blood pressures were checked. Confusion was assessed as a new disorientation in time, place or person. Specimen for complete blood count, erythrocyte sedimentation rate, fasting blood sugar electrolyte, and serum urea were collected promptly and sent to the laboratory and results were obtained. Sputum was collected in a sterile screw container. Adequacy of sputum specimen was defined as > 2 ml and containing ≤ 10 epithelial cells.[3] All samples were collected at the accident and emergency or during the time of admission. Chest radiograph was interpreted by the same radiologist and reviewed with the authors. Patients were managed based on BTS standard for the treatment of CAP.[10,12]
Data analysis
The statistical package used for data analysis is SPSS version 17.0 (Chicago, IL, USA). Data were presented in tables and charts. Sample means, standard deviation, and Chi-square test were used for statistical significance. Severity was assessed using CURB65 scoring system. Outcome of interest was 30 day mortality. In all P value of 0.05 was regarded as significant. Confidence interval was set at 95%.
Results
A total of eighty patients with diagnosis of CAP were recruited for the study as shown in Table 1. There were 39/80 (48.7%) male patients and 41/80 (51.2%) female patients with CAP. This gave male to female ratio of 1:1.05. The mean (SD) age was 56 (18.0) years. The age range was 19-89. Minimum age was 19 years while the maximum age was 89 years.
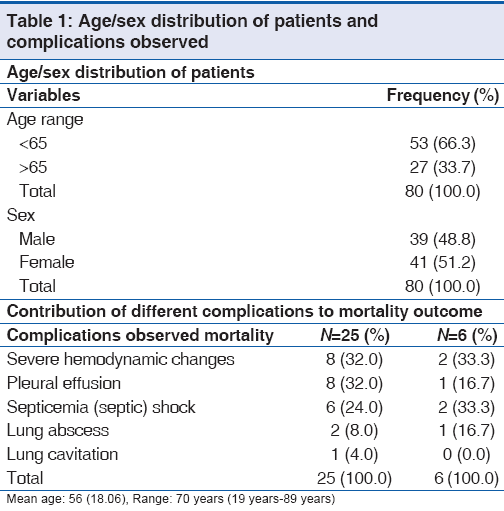
The 30 day mortality rate for those with complication was 6/25 (24%) and 6/55 (11%) in those without complication. This was not statistically significant as the Fisher exact P value was 0.1 [Table 2].
| Complications | No Complications | |
|---|---|---|
| N (%) | N (%) | |
| Mortality absent | 19 (76) | 49 (89) |
| Mortality present | 6 (24) | 6 (11) |
| Total | 25 (100) | 55 (100) |
Fisher exact: 0.120 (not significant), Odds ratio: 2.58 (0.63< OR <10.61)
Table 2: Complication and mortality in patients with community acquired pneumonia
When patients were risk stratified based on BTS guidelines mortality was found to be significantly higher in the high-risk groups (P < 0.001). On the other hand, when patients were stratified using the guideline, though complication increased with increasing risk score however, this was not statistically significant (P = 0.22) [Tables 3 and 4].
| CURB-65 score | No. of ptients N=80 | Mortlity N=12 |
|---|---|---|
| Low (score 0-1) | 44 (55) | 1 (2.2) |
| Intermedite (score 2) | 16 (20) | 2 (12.5) |
| High (score 3-5) | 20 (25) | 9 (45) |
All data are numbers (%) unless otherwise stated. χ2=19.79, P=0.001, Score 1=Low risk, 2=Moderate risk, 3-5=High risk of death from CAP
Table 3: Risk stratification using CURB-65 rule (outcome in terms of 30 day mortality)
| CURB-65 score | No. of patients | Complications |
|---|---|---|
| N=80 | N=25 | |
| Low (score 0-1) | 44 (55) | 9 (20.4) |
| Intermediate (score 2) | 16 (20) | 6 (37.5) |
| High (score 3-5) | 20 (25) | 10 (50.0) |
All data are numbers (%) unless otherwise stated. χ2=3.01, P=0.222. Score 1=Low risk, 2=Moderate risk, 3-5=High risk of death from CAP
Table 4: Risk stratification using CURB-65 rule (in terms of complications)
Mortality was higher in in-patients than out-patients however, this was not statistically significant (P = 0.33) as shown in Table 5.
| Out-patient N (%) | In-patient N (%) | |
|---|---|---|
| Mortality present | 4 (10.8) | 8 (18.6) |
| Mortality absent | 33 (89.2) | 35 (81.4) |
| Total N (%) | 37 (100.0) | 43 (100.0) |
χ2=0.95, P=0.330
Table 5: Cross tabulation of mortality in in-patients/ out-patients with community acquired pneumonia
Complications were observed in 25 patients out of 80 (31.3%) patients studied. Severe hemodynamic changes and pleural effusion were the most common complications observed in 8 patients respectively followed by septic shock which was seen in six patients. Pleural effusion ranged from mild to massive effusion. Lung cavitation was seen in one patient with klebsiella pneumonia.
Sputum culture was successful in 42/80 (52%) of cases. Micro-organisms were not isolated in 38/80 (48%) of the subjects. Streptococcus pneumonia was the most common microbial agent found in this study 14/80 (17%) [Figure 1].

Figure 1: Isolated Organisms
Discussion
In this preliminary study to determine the role of complications on the outcome of CAP in Eastern Nigeria, complications were found in (31.25%) of patients studied. Complications were found to be more common in males than in females with many elderly people developing complications. This is in agreement with other studies carried out elsewhere, which showed that both complications and risk of dying from CAP are more common in the elderly.[3,11] Sofowara et al.[4] in their study three decades ago recorded about 47% complications with mortality of about 50% in those with complications. In our study, we had less number of people with complications 25 (31.3%); with 50% of the mortality recorded in those with complications. Although, we recorded 24% mortality in our subjects with complications and this was not statistically significant. Mortality was also found to be higher in our in-patients than out-patients but this was not statistically significant [Table 5]. The higher mortality observed in admitted patients was more likely to be due to the fact that the admitted patients were more seriously ill with higher severity assessment scores with possible co-morbidities. The mortality of 18.6% in admitted patients though higher than that of out-patients, was however lower than what was found by Tanimowo[5] working in Western-Nigeria who found mortality of 26% among admitted patients. Other reason for less mortality in our study could be due to better approach to the management of CAP, especially, the use of BTS guidelines in the management of our patients.
Pleural effusion and severe hemodynamic changes were noted in 16/80 (20%) of the patients. Other complications observed were septic shock 5/80 (6.25%), lung abscess 2/80 (2.5%), and lung cavitations 1/80 (1.25%). This is in agreement with the previous works carried out, which showed that complications were common among our CAP patients, with pleural effusion being the most common complication.[2,3]
Micro-organisms infecting the lung can cause fluid accumulation in the pleural cavity. Pleural effusion can be suspected by clinical finding of stony dull percussion note on chest examination. It can be confirmed with chest X-ray, ultrasonography or chest computerized tomography (CT) scan. Our study found S. pneumonia as the most common bacterial etiology of CAP. This agreed with some other findings which implicated S. pneumonia as the most common etiology agent of CAP.[3,14,15]
Rarely bacteria in the lung will form an abscess.[16] Lung abscess can be seen with a chest X-ray, ultrasound scan or a CT scan. Abscesses typically occur in aspiration pneumonia and it is often a cause of multiple pathogens in the sputum/aspirate culture. Diagnosis of pleural effusion was both clinical and radiological, which ranged from mild to severe life threatening effusions often requiring surgical interventions. Two patients had massive effusions and one of them died.
The study by Nwosu et al.[2] showed that nearly all the patients had complications. The study took account of all the minor complications, which some authors view as normal course of the illness rather than complications.[8] Atypical organisms causing CAP can present with extrapulmonary symptoms such as jaundice, skin rashes (erythema multiforme), arthralgia or arthritis as seen in mycoplsama pneumonia. Chlamydia pneumonia can present with diarrhea, while meningismus may be seen in psittacosis as well as in C. pneumonia. These clinical features are rarely of any clinical significance when patients are stratified and well-managed.
The strength of this study lies in its prospective design, wide age range and the use of BTS guidelines in the initial assessment of patients. It is equally important to stress that all radiographs were reported by the same radiologist giving rise to less potential bias in radiological interpretation. However, this study was a prospective observational short-term study and could not look at the long-term effects of the disease on the patients; especially, those patients with complications. A larger sample size is required to support some of the conclusions made in this study.
We therefore, recommend that severity assessment using CURB-65 should be carried out for all our CAP patients and that complications should be detected early enough and managed actively by doctors treating CAP patients. We suggest a multicenter studies, which requires more funding, to be able to study the role of complications in a larger population of CAP patients and to further elucidate some of the findings in this study.
Conclusion
Mortality rate in patients with CAP though higher in patients with complications numerically were not found to be significantly higher than in those without complications. We posit that other factors like presence of higher severity assessment scores (CURB-65) and co-morbidities may be more important predictors of mortality in CAP patients and should be further studied.
Source of Support
Nil.
Conflict of Interest
None declared.
References
- Egbagbe EE, Mordi RM. Aetiology of respiratory tract infections in Benin City. J Med Biomed Res 2006;5:22-7.
- Nwosu CM, Anisuba BC. A hospital study of adults with CAP 11-clinical course and complications. Orient J Med 1991;3:196-9.
- Jennings LC, Anderson TP, Beynon KA, Chua A, Laing RT, Werno AM, et al. Incidence and characteristics of viral community-acquired pneumonia in adults. Thorax 2008;63:42-8.
- Sofowora EO, Onadeko BO. Complications and prognostic factors in pneumonia among Nigerians. Niger Med J 1973;3:144-5.
- Tanimowo MO. Mortality predictors in community-acquired pneumonia. Niger J Clin Pract 2009;12:298-301.
- Onyedum CC, Chukwuka JC. Admission profile and management of community acquired pneumonia in Nigeria – 5 year experience in a tertiary hospital. Respir Med 2011;105:298-302.
- Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. JAMA 2004;291:1238-45.
- Cunha BA. Severe community-acquired pneumonia. Crit Care Clin 1998;14:105-18.
- Rello J, Rodriguez A, Torres A, Roig J, Sole-Violan J, Garnacho-Montero J, et al. Implications of COPD in patients admitted to the intensive care unit by community-acquired pneumonia. Eur Respir J 2006;27:1210-6.
- Johnson PD, Irving LB, Turnidge JD. 3: Community-acquired pneumonia. Med J Aust 2002;176:341-7.
- BTS Standard of Care Committee. BTS Guide lines for management of CAP in adults. Thorax 2001;56:iv 1-64.
- Capelastegui A, España PP, Quintana JM, Areitio I, Gorordo I, Egurrola M, et al. Validation of a predictive rule for the management of community-acquired pneumonia. Eur Respir J 2006;27:151-7.
- Chalmers JD, Singanayagam A, Hill AT. Systolic blood pressure is superior to other haemodynamic predictors of outcome in community acquired pneumonia. Thorax 2008;63:698-702.
- Dosomu EA. Pneumonia in Nigerians. Nigerian Medical Practitioner 2002;41:65-8.
- Menéndez R, Cavalcanti M, Reyes S, Mensa J, Martinez R, Marcos MA, et al. Markers of treatment failure in hospitalised community acquired pneumonia. Thorax 2008;63:447-52.
- Pneumonia. Available from: http://www.wikipedia.org/ wiki/pneumonia [Last accessed 2009 Jan 15].



 The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.
The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.